Correspondingly, what is the difference between unstable angina and acute coronary syndrome?
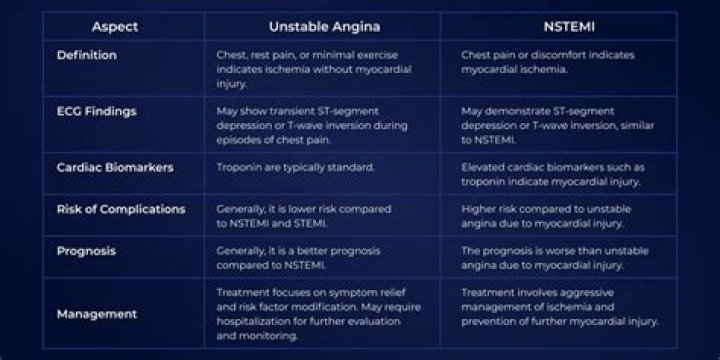
The distinguishing feature between unstable angina and non-STEMI is the presence of elevated cardiac markers, such as troponin, which implies myocardial damage. Patient history alone is insufficient to make a diagnosis of acute coronary syndrome.
Also, what is the difference between ACS and MI? Acute coronary syndrome is a term used to describe a range of conditions associated with sudden, reduced blood flow to the heart. One such condition is a heart attack (myocardial infarction) — when cell death results in damaged or destroyed heart tissue.
Hereof, what is the difference between STEMI and NSTEMI?
STEMI results from complete and prolonged occlusion of an epicardial coronary blood vessel and is defined based on ECG criteria..NSTEMI usually results from severe coronary artery narrowing, transient occlusion, or microembolization of thrombus and/or atheromatous material.
What are the 3 types of acute coronary syndrome?
Non-ST-elevation myocardial infarction (NSTEMI), ST-elevation MI (STEMI), and unstable angina are the three traditional types of ACS.
Related Question Answers
What is another name for acute coronary syndrome?
Acute Coronary Syndrome is a name given to three types of coronary artery disease that are associated with sudden rupture of plaque inside the coronary artery: Unstable angina. Non-ST segment elevation myocardial infarction or heart attack (NSTEMI) ST segment elevation myocardial infarction or heart attack (STEMI).How is unstable angina treated?
During an unstable angina event: You may get heparin (or another blood thinner) and nitroglycerin (under the tongue or through an IV). Other treatments may include medicines to control blood pressure, anxiety, abnormal heart rhythms, and cholesterol (such as a statin drug).Is atypical chest pain the same as unstable angina?
Typical (classic) angina chest pain consists of (1) Substernal chest pain or discomfort that is (2) Provoked by exertion or emotional stress and (3) relieved by rest or nitroglycerine (or both). Atypical (probable) angina chest pain applies when 2 out of 3 criteria of classic angina are present.Which artery is blocked in a STEMI?
A STEMI is a full-blown heart attack caused by the complete blockage of a heart artery.Does unstable angina show on ECG?
Unstable angina results from acute obstruction of a coronary artery without myocardial infarction. Symptoms include chest discomfort with or without dyspnea, nausea, and diaphoresis. Diagnosis is by ECG and the presence or absence of serologic markers.What does unstable angina look like on ECG?
ECG in NSTEMI & unstable angina. NSTEMI and unstable angina typically cause ST segment depressions, which are frequently accompanied by negative (inverted) T-waves or flat T-waves. Importantly, leads which display ST depressions do not necessarily reflect the ischemic area.Which is worse STEMI or NSTEMI?
NSTEMI: What You Need to Know. NSTEMI stands for non-ST segment elevation myocardial infarction, which is a type of heart attack. Compared to the more common type of heart attack known as STEMI, an NSTEMI is typically less damaging to your heart.What's worse STEMI or NSTEMI?
STEMI vs NSTEMI – Which is Worse? The bottom line is that both are just as bad. STEMI is seen as more of an immediate emergency because there is a known total occlusion of a heart vessel that needs opening back up urgently. In terms of long-term outcomes, they have equal health implications.How do you treat a STEMI?
The priority in treating a STEMI heart attack is to open the artery quickly, saving as much heart muscle as possible. Treatment options include percutaneous coronary intervention (PCI), a term that encompasses both angioplasty and stenting; clot-busting medication; and coronary artery bypass graft surgery (CABG).What causes a STEMI?
STEMI: Most commonly caused by an acute occlusion of a coronary blood vessel secondary to acute plaque rupture and thrombosis. However, cocaine use can also cause a STEMI due to coronary vasospasm, rather than occlusion with thrombosis.Is troponin elevated in NSTEMI?
Peak troponin levels were highest in STEMI, next NSTEMI, and lowest in non ACS causes. The most frequent subgroups in the non-ACS group were non-ACS cardiovascular, infectious, renal, or hypertensive causes.Is NSTEMI life threatening?
It happens when there is a complete blockage in one of your heart's major coronary arteries. It's a life-threatening emergency. It will show up as an abnormality on an electrocardiogram (EKG). NSTEMI.Can a NSTEMI lead to a STEMI?
NSTEMI rarely leads to STEMI because they have different mechanisms of action. NSTEMI is more likely in people with diffuse coronary disease, who often have collateral vessel development.How long does it take to recover from a NSTEMI?
Most patients stay in the hospital for about a week or less. Upon returning home, you will need rest and relaxation. A return to all of your normal activities, including work, may take a few weeks to 2 or 3 months, depending on your condition. A full recovery is defined as a return to normal activities.What is the problem during a myocardial infarction?
A heart attack (myocardial infarction) happens when one or more areas of the heart muscle don't get enough oxygen. This happens when blood flow to the heart muscle is blocked.What is the immediate treatment for ACS?
Morphine (or fentanyl) for pain control, oxygen, sublingual or intravenous (IV) nitroglycerin, soluble aspirin 162-325 mg, and clopidogrel with a 300- to 600-mg loading dose are given as initial treatment.What two conditions does acute coronary syndrome include?
Acute coronary syndrome is used to describe three types of coronary artery disease:- Unstable angina.
- Non-ST-segment elevation myocardial infarction or heart attack (NSTEMI)
- ST-segment elevation myocardial infarction or heart attack (STEMI)




